(303) 444-1171
MASSAGE THERAPY INTAKE FORM
CLIENT INFORMATION: All information will be kept confidential
Describe any surgeries, broken bones, major injuries or accidents below--include dates:
Please check if you have had problems with any of the following:
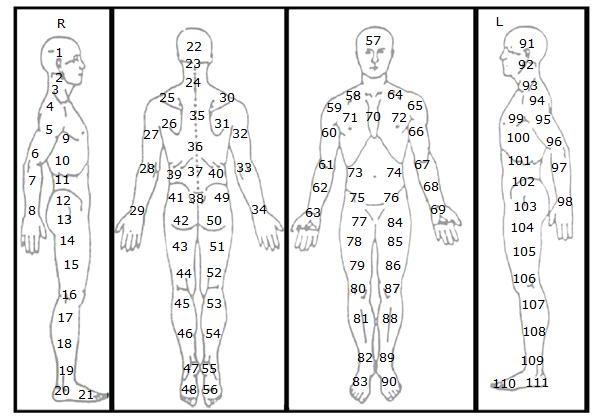
(Indicate any areas of pain or injury using the numbers in the diagrams above. Or write the name of the areas that hurt.)
PLEASE READ BEFORE SIGNING:
I understand that the treatments I receive are provided for the basic purposes of relaxation and relief of muscular tension. If I experience any pain or discomfort during my sessions, I will immediately inform the practitioner so that the pressure and/or strokes may be adjusted to my level of comfort. I further understand that our treatments should not be construed as a substitute for medical examination, diagnosis or treatment and that I should see a physician or other qualified medical specialist for any ailment that I am aware of. I understand that massage practitioners are not qualified to perform spinal or skeletal adjustments, diagnose, prescribe or treat any physical or mental illness and that nothing said in the course of the sessions given should be construed as such.
Because massage should not be performed under certain medical conditions, I affirm that I have listed all my known medical conditions and answered all questions honestly. I agree to keep my practitioners updated as to any changes in my medical profile and understand that there shall be no liability on the practitioner’s part should I fail to do so. If I have a specific medical condition or specific symptoms, massage may be contraindicated and a referral from my doctor may be required prior to service being provided. I acknowledge that on occasion, some modalities (eg. cupping, Graston/IASTM, taping, etc) may leave bruising or minor inflammation or irritation after our session, which may be a natural part of the healing process, but I will inform my practitioner immediately if this happens.
I understand that this clinic has a 24-hour cancellation policy and I will be liable for full payment for any appointments cancelled after this time. By signing below, I also authorize all employees and subcontractors of Boulder Therapeutics, Inc. to discuss and correspond about my medical status as it pertains to providing me with safe and effective massage therapy. I also understand that Boulder Therapeutics, Inc. operates within other medical and health facilities and those entities and their staff may have access to my information.
*Please select one:
I am 18 years of age or older and signing on my own behalf.
OR
I am signing as a Parent or Legal Guardian of the child listed and authorize my child to have unsupervised massage therapy (otherwise I understand that I will need to be present and in the room for the entire treatment each time).
Parent/Legal Guardian Name: Phone:
Client or Parent/Guardian Signature:
(If a minor, please have your Parent or Legal Guardian sign)
Date:
LIEN:
RE: Patient Records and Massage Therapist’s Lien
I do hereby authorize Boulder Therapeutics, Inc. to furnish you my attorney and/or insurance carrier, with a full report of my case history, examination, diagnosis, treatment, and prognosis of myself in regard to my accident/illness which occurred/began on * (date of injury).
I hereby give a lien to Boulder Therapeutics, Inc. on any settlement, claim, judgment, or verdict as a result of said accident/illness, and authorize and direct you, my attorney and/or insurance carrier, to pay directly to Boulder Therapeutics, Inc. such sums as may be due and owing them for service rendered me, and to withhold such sums from such settlement, claim, judgment, or verdict as may be necessary to protect Boulder Therapeutics, Inc. adequately.
I fully understand that I am directly and fully responsible to Boulder Therapeutics, Inc. for all medical bills submitted by them for services rendered me, and that this agreement is made solely for Boulder Therapeutics, Inc’s additional protection and in consideration of my awaiting payment. And I further understand that such payment is not contingent on any settlement, claim judgment, or verdict by which I may eventually recover said fee, unless the injured person receives a net judgment, settlement, or payment that is less than the amount of the lien, the injured person is not liable for any amount over the amount of the net judgment, settlement, or payment.
Patient Name:
Patient or Parent Guardian's Signature:
Date:
|
For Your Attorney or Insurance Carrier
The undersigned, being attorney of record or authorized representative of insurance carrier for the above patient, does hereby acknowledge receipt of the above lien, and does agree to honor the same to protect adequately Boulder Therapeutics, Inc.:
Attorney Signature: ______________________________________________________ Date: ______________
Please date, sign, and return one copy to Boulder Therapeutics, Inc. to verify
|
ASSIGNMENT OF BENEFITS
PATIENT OR PARENT/GUARDIAN:
MINOR PATIENT NAME (if applicable):
CLAIM NUMBER:
SOCIAL SECURITY NUMBER:
I hereby instruct and direct * Insurance Company to pay by check made out and mailed to:
BOULDER THERAPEUTICS, INC
1800 30TH STREET, #219
BOULDER, CO 80301
For the professional or medical expense benefits allowable and otherwise payable to me under my current insurance policy as payment toward the total charges for the professional services rendered. THIS IS A DIRECT ASSIGNMENT OF MY RIGHTS AND BENEFITS UNDER THIS POLICY. This payment will not exceed my indebtedness to the above mentioned assignee, and I have agreed to pay, in a current manner, any balance of said professional service charges over and above this insurance payment. A photocopy of this Assignment shall be considered as effective and valid as the original.
Dated:
Signature of Claimant or Policyholder:
Financial Agreement
Please read this agreement carefully. We will be happy to answer any questions you may have.
I, , (client or parent/guardian of minor client), understand that my insurance is an agreement between me and my insurance company.
I understand that Boulder Therapeutics, Inc. will assist me in billing my insurance carrier or provide a Lien to my attorney. However, I am fully responsible for any payments due that are denied by my insurance company or attorney for any reason. If copays are collected by Boulder Therapeutics, Inc., I acknowlege that those are considered to be partial payments toward full insurance billing rates and those copay amounts will be deducted from my total outstanding bill.
I assign payments to be made on my behalf to this provider for any services furnished to me. I authorize any holder of information about me to release such information needed to determine these benefits or to assist in the collection of payment for services.
If the bills for services are not paid within sixty (60) days by my insurance carrier or attorney, after a bill is presented, I am responsible for the balance on the sixty-first (61st) day, unless the settlement amount received in court is less, then we are due our pro-rata amounts.
In the event my insurance company or attorney does not pay in full for services provided, I hereby authorize the health care provider to charge all past due payments to my credit card listed below. If this card is invalid or we are unable to bill to this card for any reason, I agree to pay all past due payments within 14 days of the dated bill.
In the event fees are not paid as requested, a collection agency and possibly legal action may follow. If so, I will be responsible for all reasonable costs associated with the collection of such fees, including, but not limited to, collection costs, attorney and court costs.
I further understand that Boulder Therapeutics, Inc. has a 24-hour cancellation policy and has the right to bill me $150 for any cancellation outside of that timeframe. Unless other payment methods are arranged, I authorize Boulder Therapeutics, Inc. to charge my credit card $150 for the missed session(s).
I have read and understand this financial agreement.
Client or Parent/Guardian Signature:
Date:
*Credit Card Number:
*Exp. Date: /
*CV V:
*Name of Cardholder (as it appears on the Credit Card):
Surprise/Balance Billing Disclosure Form
(applies to health insurance only, not Auto or Worker's Compensation insurance. We are out-of-network with ALL health insurance)
Surprise Billing – Know Your Rights
Beginning January 1, 2020, Colorado state law protects you* from “surprise billing,” also known as “balance billing.” These protections apply when:
· You receive covered emergency services, other than ambulance services, from an out-of-network provider in Colorado, and/or
· You unintentionally receive covered services from an out-of-network provider at an in-network facility in Colorado
What is surprise/balance billing, and when does it happen?
If you are seen by a health care provider or use services in a facility or agency that is not in your health insurance plan’s provider network, sometimes referred to as “out-of-network,” you may receive a bill for additional costs associated with that care. Out-of-network health care providers often bill you for the difference between what your insurer decides is the eligible charge and what the out-of-network provider bills as the total charge. This is called “surprise” or “balance” billing.
When you CANNOT be balance-billed:
Emergency Services
If you are receiving emergency services, the most you can be billed for is your plan’s in-network cost-sharing amounts, which are copayments, deductibles, and/or coinsurance. You cannot be balance-billed for any other amount. This includes both the emergency facility where you receive emergency services and any providers that see you for emergency care.
Nonemergency Services at an In-Network or Out-of-Network Health Care Provider
The health care provider must tell you if you are at an out-of-network location or at an in-network location that is using out-of-network providers. They must also tell you what types of services that you will be using may be provided by any out-of-network provider.
You have the right to request that in-network providers perform all covered medical services. However, you may have to receive medical services from an out-of-network provider if an in-network provider is not available. In this case, the most you can be billed for covered services is your in-network cost-sharing amount, which are copayments, deductibles, and/or coinsurance. These providers cannot balance bill you for additional costs.
Additional Protections
· Your insurer will pay out-of-network providers and facilities directly.
· Your insurer must count any amount you pay for emergency services or certain out-of-network services (described above) toward your in-network deductible and out-of-pocket limit.
· Your provider, facility, hospital, or agency must refund any amount you overpay within sixty days of being notified.
· No one, including a provider, hospital, or insurer can ask you to limit or give up these rights.
If you receive services from an out-of-network provider or facility or agency OTHER situation, you may still be balance billed, or you may be responsible for the entire bill. If you intentionally receive nonemergency services from an out-of-network provider or facility, you may also be balance billed.
If you want to file a complaint against your health care provider, you can submit an online complaint by visiting this website: https://www.colorado.gov/pacific/dora/DPO_File_Complaint.
If you think you have received a bill for amounts other than your copayments, deductible, and/or coinsurance, please contact the billing department, or the Colorado Division of Insurance at 303-894-7490 or 1-800-930-3745.
*This law does NOT apply to ALL Colorado health plans. It only applies if you have a “CO-DOI” on your health insurance ID card.
Please contact your health insurance plan at the number on your health insurance ID card or the Colorado Division of Insurance with questions.
I am aware that Boulder Therapeutics, Inc is NOT in my health insurance’s network, including all subcontractors and all services proivded. I am voluntarily procuring their medical services with this knowledge. I understand that Boulder Therapeutics, Inc will not bill my claim(s) to my health insurance for processing. By signing, I acknowledge that I am aware that Boulder Therapeutics, Inc is out of network with ALL health insurance and that I am voluntarily receiving services with full knowledge that they are out-of-network.
Client or Parent/Guardian Signature:
(If a minor, please have your Parent or Legal Guardian sign)
(303) 444-1171
Authorization to Release Health Information
This authorization form is only required if you would like us to communcate with your medical providers.
I, , (client), authorize my Physician, and my therapists at Boulder Therapeutics, Inc., to discuss and correspond about my medical status as it pertains to providing me with safe and effective care.
I also authorize the following people to discuss and correspond about my medical status under the conditions listed here (if any). Please include phone numbers:
/
/
/
I understand that my medical records, in whole or part, will be used in this process, but that any correspondence or discussion will be confined to those medical conditions or treatments which may be affected by our treatments.
I wish to exclude the release of the items and information listed here: